From Textbook to Clinical Practice: Biliary Intervention Beyond Standard Anatomy
Sofia Bizarro-Ponte, Ana Teresa Ferreira, Filipe Craveiro, João Pedro Paulo, Andreia Rei, Isabel Pedroto, Paulo Salgueiro
Serviço de Gastrenterologia, Unidade Local de Saúde de Santo António, Porto
DESCRIPTION
An 84-year-old man with a history of gastric adenocarcinoma (pT1b N0), treated with total gastrectomy and Roux-en-Y reconstruction in 2021, presented with abdominal pain and fever. He was diagnosed with acute cholangitis and cholecystitis and subsequently underwent cholecystectomy with choledocholithiasis extraction and biliary T-tube placement. The patient was referred to our center for management of complicated choledocholithiasis (Figure 1).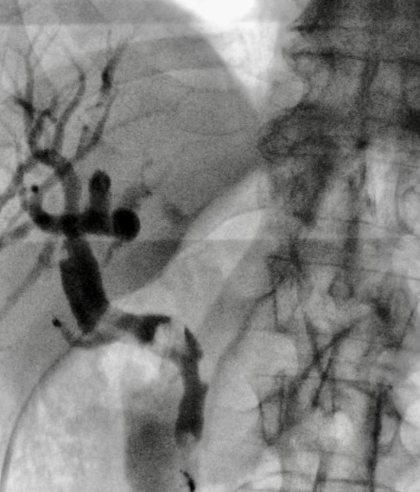
Figure 1. Choledocholithiasis
After a failed endoscopic access to the papilla, percutaneous cholangioscopy was performed through T-tube tract, after guidewire insertion and 12-Fr sheath placement (Figure 2A). A 2-cm biliary gallstone was identified (Figure 2B) and fragmented via electrohydraulic lithotripsy. Given the inaccessible papilla, an anterograde sphincteroplasty with dilation balloon was performed through the access sheath to facilitate drainage (Figure 3).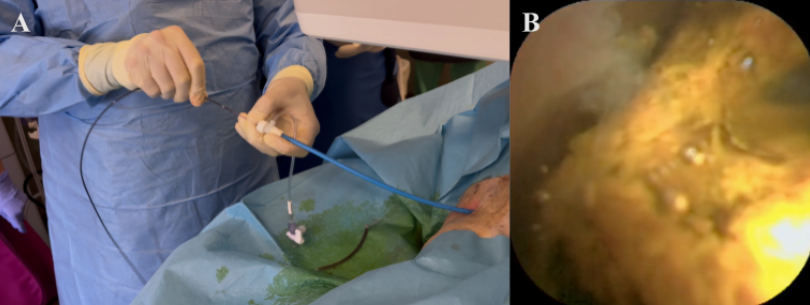
Figure 2. Introducing a SEEGEN® cholangioscope through the access sheath (A) and biliary gallstone identified through cholangioscopy
Figure 3. Anterograde sphincteroplasty with dilation balloon through the access sheath
The procedure was complicated by choleperitoneum, requiring laparoscopic peritoneal lavage and subhepatic drain placement. The patient recovered well, with drain removal one week later and discharge after an abdominal computed tomography confirmed a non-dilated and stone-free bile duct.
This case highlights the essential role of percutaneous cholangioscopy in managing complex cholelithiasis in patients with altered anatomy and no endoscopic access. Through a percutaneous approach, direct visualization and effective lithotripsy were achieved, overcoming Roux-en-Y anatomical challenges. Despite being complicated by biliary leakage, in this case, surgery was minimally invasive, without the need of biliary re-intervention.
REFERENCES
1. Anjum, M.R., Dyer, J., Curran, F., et al. Cholangioscopy-guided electrohydraulic lithotripsy of a large bile duct stone through a percutaneous T-tube tract. VideoGIE. 2018 Oct 25;3(12):390-391. doi: 10.1016/j.vgie.2018.09.001. PMID: 30506004; PMCID: PMC6251702.
2. Bower, B.L., Picus, D., Hicks, M.E., et al.Choledochoscopic Stone Removal through a T-Tube Tract: Experience in 75 Consecutive Patients. Journal of Vascular and Interventional Radiology, Volume 1, Issue 1, 1990, Pages 107-112, ISSN 1051-0443. doi:10.1016/S1051-0443(90)72513-4.
3. Zhang, L., Li, L., Yao, J. et al. Residual choledocholithiasis after choledocholithotomy T-tube drainage: what is the best intervention strategy?. BMC Gastroenterol 22, 509 (2022). doi:10.1186/s12876-022-02601-6
4. Clarete, A., Nasner, D., Toro-Gutiérrez, J.S., et al. Successful application of percutaneous endoscopic cholangioscopy + electrohydraulic lithotripsy for hepatolithiasis post-liver transplantation: a case report. J Med Case Rep. 2024 Sep 27;18(1):472. doi: 10.1186/s13256-024-04669-y. PMID: 39334321; PMCID: PMC11429367.