Hidden diagnosis - not all subepithelial lesions are what you expect
Mónica Francisco, Sofia Bragança, Fábio Pereira Correia, David Horta, Joana Carvalho Branco
Hospital Professor Doutor Fernando Fonseca
DESCRIPTION
A 57 year old man presented with upper gastrointestinal bleeding, associated with a 3-month history of unintentional weight loss (18% of body weight) and anorexia. Upper endoscopy revealed a 4 cm subepithelial lesion in the gastric corpus, partially ulcerated, raising clinical suspicion of a gastrointestinal stromal tumor (GIST). Due to the lesion's location and nature, definitive endoscopic treatment was not feasible. Abdominal CT scan showed a large mass (16 x 9 cm) in the gastric fundus with central necrosis, invading the spleen and pancreatic tail, along with perilesional lymphadenopathy and multiple hypodense hepatic nodules. Due to the high risk of bleeding, the patient underwent hemostatic radiotherapy, and one liver nodule was biopsied for histologic diagnosis. Surprisingly, the biopsy showed a neuroendocrine tumor (NET) G2. To confirm the diagnosis of the gastric lesion, an endoscopic ultrasound was performed, revealing a large hypoechoic lesion, invading surrounding organs with perilesional lymphadenopathy. Identification of origin layer was not possible. A 22G fine needle biopsy (FNB) confirmed a diagnosis of neuroendocrine tumor G3 (Ki67 61%).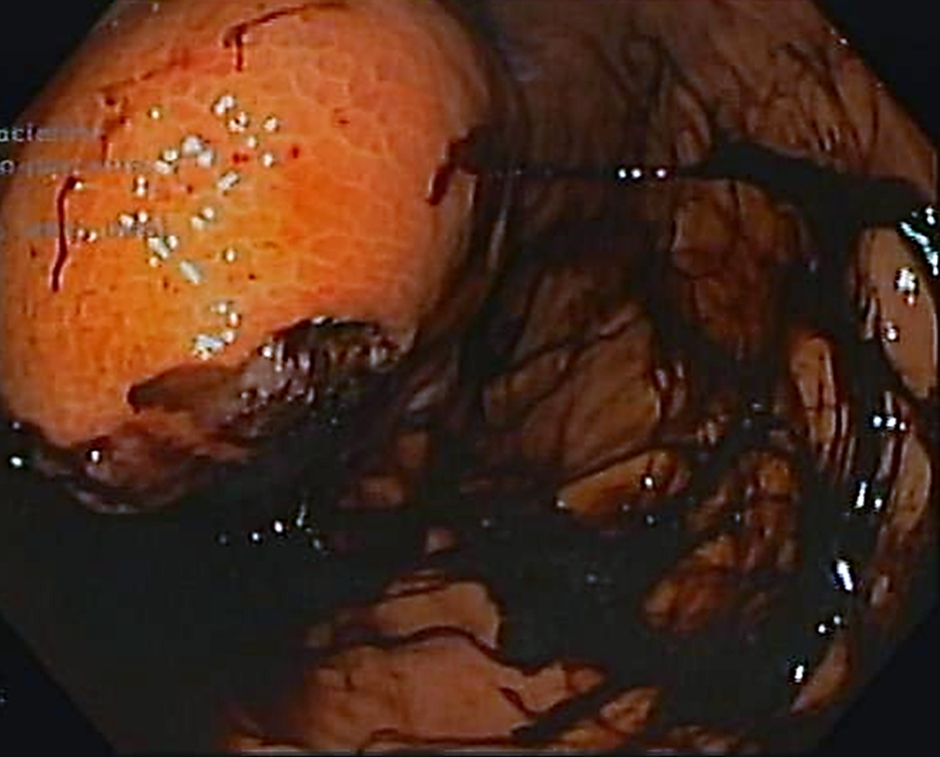 Figure 1. Endoscopic image of the gastric subepithelial lesion.
Figure 1. Endoscopic image of the gastric subepithelial lesion.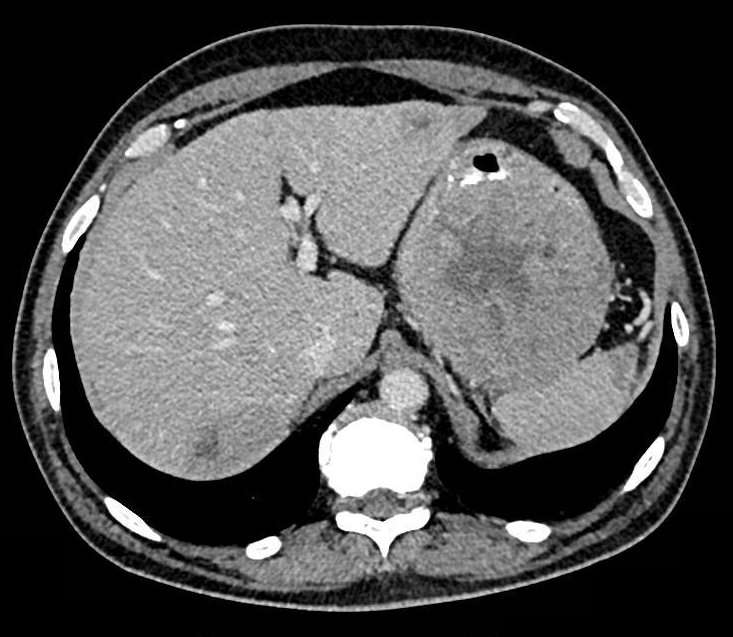 Figure 2. CT scan image showing large gastric lesion with central necrosis and two liver metastasis.
Figure 2. CT scan image showing large gastric lesion with central necrosis and two liver metastasis.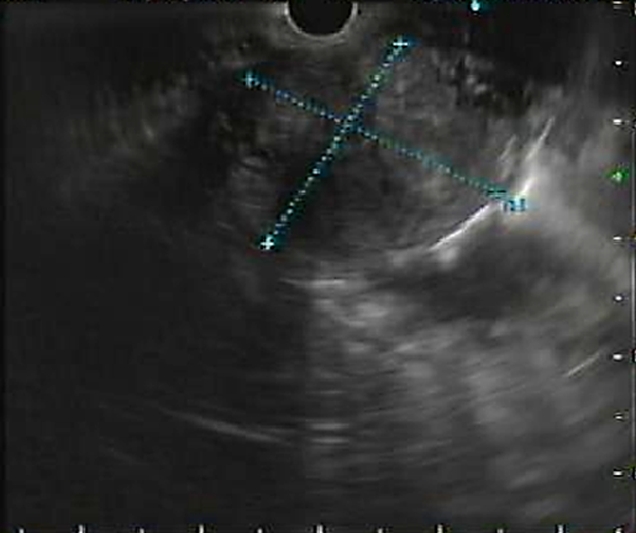 Figure 3. Ultrasonographic image of gastric lesion.
Figure 3. Ultrasonographic image of gastric lesion.
DISCUSSION
NETs are rare neoplasms, with gastric NETs being the most common among the digestive tract. They usually present as yellowish polypoid lesions with an occasional central depression or ulceration, and are commonly associated to chronic autoimmune gastritis. More infrequently (less than 20%), sporadic NETs may present as subepithelial lesion. However, when a large (>5cm) subepithelial lesion presents with gastrointestinal bleeding, a GIST is often empirically suspected. Furthermore, the presence of metastatic disease with G2 histology demanded histologic confirmation of the gastric lesion, in order to exclude a metachronous neoplasm, for which endoscopic ultrasound is an essential tool.
REFERENCES
- Carvão J, Dinis-Ribeiro M, Pimentel-Nunes P, Libânio D. Neuroendocrine Tumors of the Gastrointestinal Tract: A Focused Review and Practical Approach for Gastroenterologists. GE Port J Gastroenterol. 2021;28(5):336-348. doi:10.1159/000512089
- Lee J, Oh SJ. Gastric Neuroendocrine Tumor Mimicking Gastrointestinal Stromal Tumor: A Case Report. Case Rep Oncol. 2021;14(3):1271-1276. Published 2021 Sep 6. doi:10.1159/000518078
- Kim Y, Ahn B, Choi KD, et al. Gastric Neuroendocrine Tumors According to the 2019 World Health Organization Grading System: A Single-Center, Retrospective Study. Gut Liver. 2023;17(6):863-873. doi:10.5009/gnl220175